
Human Papillomavirus (HPV): Understanding for Comprehensive Health Protection
Human Papillomavirus (HPV) is a group of common viruses affecting millions worldwide. With the ability to cause various health issues, from genital warts to serious cancers, understanding HPV is essential for protecting individual and community health. This comprehensive guide covers the introduction, consequences, transmission, diagnosis, treatment, vaccination, monitoring, and the link to other sexually transmitted infections (STIs).
1. General Introduction to HPV
Human Papillomavirus (HPV) is the collective name for a group of over 200 related viruses. It is the most common sexually transmitted infection (STI) in the world. Most sexually active people will contract at least one type of HPV at some point in their lives, often without clear symptoms. HPV can affect the skin, genital area, and throat. HPV strains are classified into two main groups based on disease risk: low-risk and high-risk. Low-risk HPV types often cause genital warts and respiratory papillomatosis. Among these, HPV 6 and 11 are the two most common types, responsible for about 90% of genital wart cases. Conversely, high-risk HPV types (cancer-causing) have the potential to cause precancerous cell changes and cancer. At least 12 high-risk HPV types have been identified, with HPV 16 and 18 being the two most common, causing about 70% of cervical cancer cases globally. Other high-risk types include 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59. HPV is so common that almost all men and women will be infected with at least one type of HPV in their lifetime. In the United States, an estimated 14 million new infections occur each year. The body’s immune system usually clears the virus on its own within 1–2 years in about 90% of cases, regardless of whether it is a low-risk or high-risk type. The widespread prevalence of HPV, coupled with the fact that the majority of infections are asymptomatic, indicates that contracting the virus is not a sign of personal irresponsibility or “promiscuous” sexual behavior. This is important to reduce stigma and encourage individuals, including those in high-risk groups such as women who start sexual activity early, those with genital warts, sex workers, and MSM, to proactively seek information, testing, and vaccination without fear of judgment or evaluation.
2. Consequences of HPV Infection: From Genital Warts to Cancer
HPV infection can lead to various health consequences, ranging from benign lesions like genital warts to dangerous types of cancer. Clearly distinguishing between these types of lesions is very important for a correct understanding of the risks and management approaches.
2.1. Genital Warts: Manifestation and Association with HPV
Genital warts are rough papules, which can be flat or raised, shaped like small cauliflower or fleshy bumps. They commonly appear in the genital area, including the vulva, vagina, and cervix in women, and the penis, scrotum, and anus in men. In some rare cases, they can also appear in the mouth or throat. These warts may appear weeks, months, or even years after infection. Genital warts are mainly caused by low-risk HPV strains like HPV 6 and 11, which account for about 90% of cases. Although genital warts are usually not painful, they can cause itching, discomfort, or bleeding. It is important to note that genital warts are not directly life-threatening and do not progress to cancer. However, they can cause significant discomfort, psychological stress, and shame for the patient. Clearly distinguishing between HPV that causes genital warts (low-risk) and HPV that causes cancer (high-risk) is very important. This helps reassure patients with genital warts that they do not necessarily face a cancer risk, while also emphasizing that the absence of genital warts does not mean there is no cancer risk, because high-risk HPV strains often do not cause clear symptoms.
2.2. HPV and Cancer Risk
Persistent high-risk HPV infection can lead to many types of cancer in both men and women. The main HPV-related cancers include:
- Cervical Cancer: Nearly all cases of cervical cancer are caused by HPV. This is the fourth most common cancer in women globally.
- Anal Cancer: More than 90% of anal cancer cases are caused by HPV.
- Vulvar and Vaginal Cancer: About 69-75% of vulvar and vaginal cancer cases are associated with HPV.
- Penile Cancer: About 60-63% of penile cancer cases are caused by HPV.
- Oropharyngeal Cancer (Throat Cancer): About 60-70% of oropharyngeal cancer cases (including the base of the tongue, tonsils, and back of the throat) may be linked to HPV, although factors like tobacco and alcohol also play important roles.

The most common high-risk HPV strains causing cancer are HPV 16 and 18, but other strains like 31, 33, 45, 52, 58 are also high-risk. The progression from persistent infection to precancerous lesions and cancer occurs as follows: When the immune system cannot clear a high-risk HPV infection, the virus can persist in the body. This persistent infection can cause abnormal cell changes, known as dysplasia or precancerous lesions (e.g., CIN – cervical intraepithelial neoplasia, VIN – vulvar intraepithelial neoplasia, AIN – anal intraepithelial neoplasia, PeIN – penile intraepithelial neoplasia). If not detected and treated, these changes can progress to cancer after many years or even decades. For example, cervical cancer can take 15-20 years to develop after HPV infection. The long incubation period of HPV before causing cancer provides an important opportunity for secondary prevention strategies through screening. This emphasizes that periodic screening is not just about early cancer detection but also about cancer prevention by removing precancerous lesions before they have a chance to develop into malignancy. For high-risk groups, understanding this process will encourage them to adhere to the periodic screening schedule for timely detection and intervention.
Table 1: HPV Types and Diseases Caused
| HPV Type | Common Strains | Main Diseases Caused | Danger Level |
|---|---|---|---|
| Low Risk | HPV 6, 11 | Genital warts, respiratory papillomatosis | Not life-threatening, not cancer-causing, but can cause discomfort and psychological stress. |
| High Risk | HPV 16, 18, 31, 33, 45, 52, 58 | Cervical cancer, anal cancer, penile cancer, vulvar cancer, vaginal cancer, oropharyngeal cancer (throat cancer) | Potential to cause cancer if infection is persistent and left untreated. |
3. How is HPV Transmitted?
HPV is primarily transmitted through intimate skin-to-skin contact, including vaginal, anal, and oral sex. The virus can spread from one genital area to another, or from the hand to the genital area. In some rare cases, HPV can also be transmitted from mother to child during childbirth.

An important characteristic of HPV is its ability to transmit even when the infected person has no signs or symptoms. This makes it difficult to determine the time and source of the initial infection. Therefore, a person may have been infected with HPV for many years without knowing it. Regarding the role of condoms in reducing transmission risk, correct and consistent condom use can reduce the risk of contracting and transmitting HPV, as well as developing HPV-related diseases (such as genital warts or cervical cancer). However, condoms do not provide complete protection because HPV can infect areas of the skin not covered by the condom, such as the scrotum or anus. The fact that condoms do not completely protect against HPV is important information so that readers do not have a false sense of security. This emphasizes that condoms, although important for preventing other STIs, are not the only solution for HPV. It reinforces the message that vaccination is the most effective preventive measure, supplementing other safe sexual practices, especially for high-risk groups.
4. Diagnosis of HPV Infection and Related Lesions
Diagnosis of HPV and related lesions is an essential step for managing and preventing the serious consequences of the virus. Diagnostic methods include both routine screening tests and advanced procedures when necessary.
4.1. HPV Testing Methods
- Pap Test (Pap smear):
- Purpose: To look for abnormal or precancerous cells on the cervix that could develop into cervical cancer if not treated.
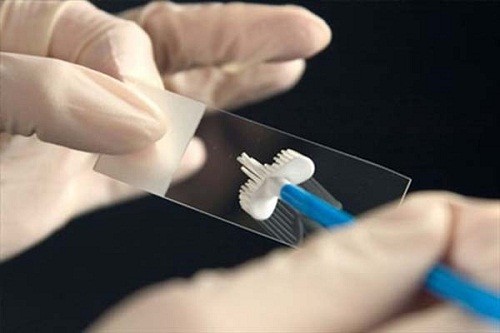
- Procedure: During a pelvic exam, the doctor will use a speculum to view the vagina and cervix, and then use a small brush or swab to collect a few cells and mucus from the cervix. This cell sample is then sent to a laboratory for examination under a microscope.
- Result Interpretation:
- Normal/Negative: No abnormal cells found; this is a good result.
- Atypical/Undetermined Significance (ASC-US): Cervical cells look somewhat abnormal, but it’s unclear if they are related to HPV. This could be due to other factors such as pregnancy, menopause, or infection.
- Abnormal/Positive: Abnormal cells are found. This result does not mean cancer is immediately present but may indicate a precancerous condition. Further testing or follow-up is needed as recommended by the doctor.
- Unsatisfactory: The sample did not contain enough cells or was obscured by blood/mucus; the test needs to be repeated after a few months.
- HPV DNA Test:
- Purpose: To look for the DNA of high-risk HPV strains (cancer-causing) in a cervical cell sample.
- Procedure: Similar to the Pap test, a cell sample is collected from the cervix. In some cases, the patient may self-collect the sample at home with the doctor’s instructions. The sample is then sent to a molecular biology laboratory for analysis.
- Result Interpretation:
- Negative: No high-risk HPV found. This indicates a low risk of developing HPV-related cervical cancer.
- Positive: High-risk HPV DNA is found. This result does not mean cancer is immediately present but indicates a high-risk HPV infection, which increases the risk of developing precancerous lesions or cervical cancer in the future. Further monitoring or testing is needed as recommended by the doctor.
- Co-testing: Is the simultaneous performance of both the Pap test and the HPV DNA test. This method helps increase the accuracy of screening. If both results are normal, the interval for periodic screening can be extended to 5 years.
- Visual Diagnosis of Genital Warts: Genital warts are usually diagnosed based on a visual examination by a doctor. A biopsy may be performed if the diagnosis is uncertain, the lesion does not respond to treatment, or there are other abnormal signs.
4.2. Advanced Diagnostic Procedures
When screening test results (Pap or HPV DNA) show abnormalities, the doctor may order advanced diagnostic procedures for a more detailed evaluation.
- Colposcopy:
- Purpose: To thoroughly examine the cervix, vagina, and vulva using a magnifying device with light (colposcope) to look for abnormal cell areas not visible to the naked eye.
- Procedure: The doctor inserts a speculum into the vagina, then applies a vinegar solution (acetic acid) to the cervix. This solution helps highlight abnormal cell areas by making them turn white. The doctor then observes through the colposcope.
- Biopsy:
- Purpose: To take a small sample of cells or tissue from the cervix (or other areas with suspicious lesions) for examination under a microscope, to accurately determine the degree of cell abnormality and rule out cancer.
- Common Biopsy Types:
- Loop Electrosurgical Excision Procedure (LEEP): This is a procedure that uses a thin wire loop with an electric current to remove abnormal tissue. LEEP is often performed in the clinic with local anesthesia and takes only a few minutes.
- Cold Knife Conization: This procedure uses a scalpel to remove a cone-shaped piece of tissue from the cervix. Cold knife conization is typically performed in a hospital under general anesthesia.
- Biopsy is not only used for diagnosis but can also be used as a treatment method, completely removing precancerous tissue.
Understanding the diagnostic methods allows patients to be more proactive in monitoring their health. Especially for women, knowing that the Pap and HPV tests can detect precancerous conditions before they become cancer is a powerful message. This encourages them to adhere to the periodic screening schedule, helping to detect cell changes early and intervene promptly, thereby preventing the development of cancer.
5. Treatment of HPV and Related Conditions
Currently, there is no cure for the HPV virus. However, the body usually clears the virus on its own within 1-2 years for the majority of infections. Treatment mainly focuses on removing the lesions caused by HPV, such as genital warts or precancerous cells.
5.1. Treatment of Genital Warts
The main goal of genital wart treatment is to remove visible lesions, reduce symptoms (itching, pain, discomfort), and improve aesthetics. If they do not cause discomfort, genital warts may not require treatment and may disappear on their own, remain the same, or grow in size and number. Treatment methods include:
- Topical Treatments (Creams):
- Common over-the-counter wart treatments should not be self-applied for genital warts as they are not intended for this sensitive area.
- Removal Procedures: For larger warts or those that do not respond to topical medication, the following procedures may be indicated:
- Cryotherapy (Áp lạnh): Freezing the warts with liquid nitrogen, which creates a blister around the wart. When the skin heals, the wart falls off. This method may need to be repeated multiple times.
- Electrocautery (Đốt điện): Using an electric current to burn off the warts.
- Laser: Using a high-intensity light beam to destroy the warts. This method is usually reserved for widespread and difficult-to-treat cases of genital warts.
- Surgical Excision (Phẫu thuật cắt bỏ): Cutting out the warts with a scalpel. This procedure is performed under local or general anesthesia.
- Loop Electrosurgical Excision Procedure (LEEP): In addition to diagnosis, LEEP is also used to remove genital warts or abnormal cells.
Genital warts may recur after treatment.
5.2. Treatment of Precancerous Lesions
For precancerous lesions caused by HPV, especially in the cervix (CIN), management and treatment depend on the severity of the lesion.
- Monitoring and Management of Low-Grade Lesions (CIN 1): Mild cell changes (CIN 1) often disappear on their own and do not require immediate treatment. The doctor may recommend periodic monitoring with Pap and/or HPV DNA tests to ensure the lesion does not progress.
- Methods for Removing Precancerous Lesions (CIN 2, CIN 3): Moderate (CIN 2) or severe (CIN 3) lesions are at high risk of progressing to cancer if left untreated. Although CIN 2 can sometimes resolve on its own, CIN 3 requires immediate treatment (unless pregnant). Treatment methods are similar to genital wart removal procedures but focus on removing abnormal cells on the cervix:
- Loop Electrosurgical Excision Procedure (LEEP): Is a common procedure to remove precancerous lesions on the cervix. This procedure removes a thin layer of abnormal tissue and can also provide a biopsy sample for diagnostic confirmation.
- Cold Knife Conization (Khoét chóp lạnh): Similar to LEEP, but uses a scalpel to remove tissue. It is usually performed when a larger tissue sample is needed or in more complex cases.
- Thermal Ablation (Đốt nhiệt): WHO recommends using thermal ablation to treat precancerous lesions of the cervix.
Early detection of precancerous lesions through periodic screening and timely treatment is very important to prevent them from developing into invasive cancer. Although there is no cure for the HPV virus, effective management of lesions caused by the virus can help maintain health and prevent serious complications.
6. HPV Prevention with Vaccination
Vaccination is the most effective method to prevent HPV infection and related diseases, including cancer and genital warts.
6.1. HPV Vaccine: Types and Effectiveness
Currently, the HPV vaccine licensed and widely used is the 9-valent vaccine (Gardasil 9). This vaccine protects against 9 HPV types:
- HPV 6 and 11: Two low-risk types that cause about 90% of genital wart cases.
- HPV 16, 18, 31, 33, 45, 52, and 58: Seven high-risk types responsible for the majority of cervical cancer cases and other HPV-related cancers. HPV 16 and 18 alone cause about 70% of cervical cancer.
The effectiveness of the HPV vaccine is very high, especially when administered before exposure to the virus (before starting sexual activity). Clinical studies have demonstrated up to 99% effectiveness in preventing severe precancerous lesions caused by HPV 16/18 and 99% effectiveness in preventing genital warts caused by HPV 6/11/16/18. The vaccine may also provide a certain degree of cross-protection against high-risk HPV types not included in the vaccine. The highest vaccine effectiveness is recorded in the younger age group (9-14 years old).
6.2. HPV Vaccination Schedule for Males and Females
Major health organizations like the CDC and WHO recommend the HPV vaccine for both males and females to effectively prevent the disease.
- Recommended Age:
- Routine Vaccination: Recommended to administer the vaccine to children at age 11 or 12. Vaccination can start as early as age 9. Vaccination at this age is proven to be most effective because it is usually before the child becomes sexually active and is exposed to the virus.
- Catch-up Vaccination: Recommended for individuals aged 13 to 26 who were not fully vaccinated when they were younger.
- Adults Aged 27 to 45: Current studies have shown the benefit of HPV vaccination even after age 27, so there is no age limit for HPV vaccination.
- Number of Doses and Interval Between Doses:
- 2-Dose Schedule: For most people starting vaccination at ages 9 to 14. The second dose is given 6 to 12 months after the first dose. WHO has also considered the possibility of a single dose as an optional regimen for the 9-20 age group, based on equivalent efficacy and duration of protection as the two-dose regimen.
- 3-Dose Schedule: For those starting vaccination at ages 15 to 45, and for immunocompromised individuals (regardless of age at vaccination start). The schedule is 0, 1-2, 6 months.
- Benefits of Vaccination for Both Males and Females:
- For Females: The vaccine helps prevent cervical cancer, vulvar cancer, vaginal cancer, and genital warts.
- For Males: The vaccine helps prevent penile cancer, anal cancer, oropharyngeal cancer, and genital warts.
- Vaccinating males also plays an important role in reducing HPV transmission in the community, creating a herd immunity effect and indirectly protecting females.
6.3. Safety and Side Effects of the HPV Vaccine
The HPV vaccine is considered safe and highly effective. Vaccine safety monitoring systems and over 160 studies have demonstrated the favorable safety profile of the HPV vaccine.
- Common Side Effects: Most side effects are mild and transient, including pain, redness, or swelling at the injection site, fever, headache, fatigue, nausea, and muscle or joint pain.
- Serious Side Effects: Severe allergic reactions after vaccination are very rare but can be life-threatening. Fainting can also occur after vaccination, including the HPV vaccine.
- Notes on Vaccination:
- Pregnant Women: The HPV vaccine is not recommended for use in pregnant women.
- Immunocompromised Individuals: People with a weakened immune system (e.g., those with HIV/AIDS, organ transplant recipients, or those using certain immunosuppressive drugs) may need a 3-dose vaccine regimen to achieve optimal protection.
- Allergies: Individuals with a history of severe allergic reaction (e.g., anaphylaxis) to a previous dose of the vaccine or to any vaccine components (including yeast) should not receive the HPV vaccine.
HPV vaccination is an important tool for preventing cancer and diseases related to HPV. It helps create a strong protective shield, especially when administered at the recommended age, before likely exposure to the virus.
7. Monitoring HPV Infection and High-Risk Individuals
Periodic monitoring is extremely important for individuals who have contracted HPV, especially high-risk groups, even if they have been vaccinated.
- The Importance of Routine Screening (Pap, HPV test) Even After Vaccination: Although the HPV vaccine is very effective in preventing the most common cancer-causing HPV strains, the vaccine does not protect against all HPV strains that can cause cancer, nor does it treat pre-existing HPV infections. Therefore, vaccinated women still need to continue routine cervical cancer screening (Pap and/or HPV DNA testing) as recommended by their doctor.
- Monitoring Guidelines for Individuals with HPV Infection:
- For most HPV infections, the body’s immune system will clear the virus within 1-2 years without causing any health problems.
- If the HPV DNA test result is positive for a high-risk strain, this does not mean cancer is present, but it indicates a higher risk of developing precancerous lesions or cancer in the future. The doctor will recommend specific follow-up steps, which may include colposcopy and/or biopsy for a more detailed evaluation of the cervical cells.
- Individuals with a history of precancerous lesions (e.g., CIN 2, CIN 3) need to continue monitoring for at least 25 years after the lesion is detected, even after age 65.
- Special Notes for High-Risk Individuals: Some groups of people are at a higher risk of developing persistent HPV infection and related diseases, and therefore need closer monitoring:
- People with HIV/AIDS: The immune system weakening due to HIV significantly increases the risk of persistent HPV infection and progression to cancer, especially cervical and anal cancer. Women with HIV should be screened for cervical cancer more frequently, for example, every 3 years starting from age 25. For people with HIV, a 3-dose HPV vaccine regimen is recommended.
- Immunocompromised Individuals: Including organ transplant recipients, people with autoimmune diseases like systemic lupus erythematosus, or those using immunosuppressive drugs. This group also needs more frequent screening as recommended by their doctor.
- Men Who Have Sex with Men (MSM): MSM have a higher risk of high-risk HPV infection and developing anal cancer. Anal cancer screening (e.g., Anal Pap test) may be recommended for this group.
- Sex Workers: Due to the nature of their work and the number of partners, this group has a high risk of contracting multiple types of HPV and other STIs and needs access to regular screening and vaccination services.
- Women Who Start Sexual Activity Early: A young age at first sexual intercourse can increase the risk of developing cervical cancer if infected with HPV.
Understanding risk factors and adhering to periodic monitoring guidelines is key to early detection and effective management of HPV-related health issues, especially in vulnerable populations.
8. HPV and Co-infection with Other STIs
HPV infection often occurs simultaneously with other sexually transmitted infections (STIs). This co-infection can affect the disease course, the risk of developing complications, and even fertility. Evidence shows a higher prevalence of HPV in people co-infected with other STIs. For example, the co-infection rate of HPV with agents such as Ureaplasma urealyticum, Ureaplasma parvum, Chlamydia trachomatis, Mycoplasma genitalium, Herpes simplex virus 2, Neisseria gonorrhoeae, Enterococcus faecalis, and Staphylococcus aureus has been noted. The link between HPV and other STIs can be explained by the following factors:
- Common Transmission Route: STIs are often transmitted through the same route (unsafe sexual contact); therefore, contracting one STI increases the likelihood of exposure and infection with other STIs.
- Impact on Local Immunity: Some STIs can cause inflammation or damage to the mucous membranes, creating favorable conditions for the HPV virus to invade and persist.
- Systemic Immunodeficiency: In particular, Human Immunodeficiency Virus (HIV) infection is a major risk factor for persistent HPV infection and disease progression. The weakened immune system due to HIV reduces the body’s ability to clear HPV, leading to higher rates of HPV infection, especially high-risk strains like HPV 16 and 18, and accelerates the progression to precancerous lesions and cancer (e.g., cervical cancer).
The impact of co-infection on health can be varied:
- Disease Progression: Co-infection with STIs can increase the risk of progression of HPV-related precancerous lesions.
- Male Infertility: Studies have indicated that HPV infection alone can significantly reduce semen volume and total sperm count. Furthermore, HPV co-infection with agents like Ureaplasma urealyticum can significantly reduce sperm motility and viability, emphasizing the necessity of STI screening in semen for infertile men.
In summary, co-infection between HPV and other STIs is a complex health issue, especially in high-risk groups. Awareness of this connection is necessary to implement comprehensive prevention and effective medical management.
9. Conclusion
The HPV virus is an extremely common sexually transmitted agent with the potential to cause many serious health issues, from genital warts to various cancers such as cervical, anal, penile, vulvar, vaginal, and oropharyngeal cancer. Although most HPV infections resolve on their own, persistent infection with high-risk strains can lead to precancerous lesions and cancer after many years. To protect overall health from HPV, proactively implementing prevention and monitoring measures is extremely important:
- HPV Vaccination: This is the most effective preventive measure, recommended for both males and females aged 9-26. For adults aged 27-45, vaccination is still beneficial, and there is no age limit for vaccination. Vaccination before sexual activity provides optimal protection.
- Routine Screening: For women, routine Pap and/or HPV DNA testing is essential for the early detection of abnormal or precancerous cells, even after vaccination. Early detection allows for timely intervention, preventing the disease from progressing to cancer.
- Practicing Safe Sex: Correct and consistent condom use can reduce the risk of HPV transmission and other STIs, although it does not provide complete protection against HPV. Limiting the number of partners is also a way to reduce risk.
- Medical Consultation: If there are any abnormal symptoms (such as genital warts) or abnormal screening results, it is necessary to promptly consult a doctor for timely diagnosis and treatment. High-risk groups (women who start sexual activity early, those with genital warts, sex workers, MSM, people with HIV or compromised immunity) need to pay special attention to periodic monitoring and screening as recommended by health experts.
Understanding HPV and being proactive in prevention, early detection, and management of the disease not only helps protect individual health but also contributes to reducing the burden of disease for the community.
This article is written by Dr Đỗ Hữu Đạt. The doctor has many years of in-depth experience in reproductive and sexual health care.
Reference
- [1]. Human papillomavirus and cancer – World Health Organization (WHO), https://www.who.int/news-room/fact-sheets/detail/human-papilloma-virus-and-cancer
- [2]. HPV and Cancer – NCI, https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer
- [3]. Human Papillomavirus (HPV) Vaccine Safety | Vaccine Safety | CDC, https://www.cdc.gov/vaccine-safety/vaccines/hpv.html
- [4]. HPV (Human Papillomavirus): Causes, Symptoms & Treatment, https://my.clevelandclinic.org/health/diseases/11901-hpv-human-papilloma-virus
- [5]. Genital HPV Infection – CDC Fact Sheet. – DPBH, https://dpbh.nv.gov/uploadedFiles/dpbh.nv.gov/content/Programs/STD/dta/Publications/HPV.pdf
- [6]. Human Papillomavirus (HPV) Vaccine – PAHO/WHO | Pan American Health Organization, https://www.paho.org/en/human-papillomavirus-hpv-vaccine
- [7]. Human Papillomavirus (HPV), HPV-Related Disease, and the HPV …, https://pmc.ncbi.nlm.nih.gov/articles/PMC2492590/
- [8]. Basic Information about HPV and Cancer | Cancer | CDC, https://www.cdc.gov/cancer/hpv/basic-information.html
- [9]. Human Papillomavirus Epidemiology and Prevention: Is There Still a Gender Gap? – PMC, https://pmc.ncbi.nlm.nih.gov/articles/PMC10303003/
- [10]. HPV Vaccine Administration – CDC, https://www.cdc.gov/vaccines/vpd/hpv/hcp/administration.html
- [11]. Dosing Schedules and Administration of GARDASIL®9 (Human Papillomavirus 9-valent Vaccine, Recombinant) – MerckVaccines.com, https://www.merckvaccines.com/gardasil9/dosing-administration/
- [12]. Impact of human papillomavirus vaccines in the reduction of infection, precursor lesions, and cervical cancer: A systematic literature review, https://pmc.ncbi.nlm.nih.gov/articles/PMC12153211/
- [13]. HPV infection – Symptoms & causes – Mayo Clinic, https://www.mayoclinic.org/diseases-conditions/hpv-infection/symptoms-causes/syc-20351596
- [14]. Human Papillomavirus (HPV) Statistics | Did You Know? – YouTube, https://www.youtube.com/watch?v=I1LrOWwIgCg&pp=0gcJCfwAo7VqN5tD
- [15]. HPV and Pap Test Results: Next Steps after an Abnormal Cervical Cancer Screening Test, https://www.cancer.gov/types/cervical/screening/abnormal-hpv-pap-test-results
- [16]. Human Papillomavirus (HPV) Test: MedlinePlus Medical Test, https://medlineplus.gov/lab-tests/human-papillomavirus-hpv-test/
- [17]. Human Papillomavirus (HPV) Infection – STI Treatment Guidelines – CDC, https://www.cdc.gov/std/treatment-guidelines/hpv.htm
- [18]. Screening for Cervical Cancer – CDC, https://www.cdc.gov/cervical-cancer/screening/index.html
- [19]. The American Cancer Society Guidelines for the Prevention and Early Detection of Cervical Cancer, https://www.cancer.org/cancer/types/cervical-cancer/detection-diagnosis-staging/cervical-cancer-screening-guidelines.html
- [20]. Cancer – World Health Organization (WHO), https://www.who.int/news-room/fact-sheets/detail/cancer
- [21]. Cervical cancer screening in high-risk patients: Clinical challenges in primary care, https://www.ccjm.org/content/91/11/693
- [22]. SECTION 6: PROCEDURES FOR HPV TEST SAMPLE COLLECTION AND SHIPMENT TO THE LABORATORY – PAHO, https://www3.paho.org/hq/dmdocuments/2016/manual-VPH-English-06.pdf
- [23]. Genital Warts, https://www.dph.ncdhhs.gov/media/3413/open
- [24]. Genital warts – Diagnosis and treatment – Mayo Clinic, https://www.mayoclinic.org/diseases-conditions/genital-warts/diagnosis-treatment/drc-20355240
- [25]. Introduction – WHO guideline for screening and treatment of cervical pre-cancer lesions for cervical cancer prevention – NCBI, https://www.ncbi.nlm.nih.gov/books/NBK604767/
- [26]. Human Papillomavirus Disease: Adult and Adolescent OIs | NIH – Clinical Info HIV.gov, https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-opportunistic-infections/human
- [27]. Optimizing HPV vaccine effectiveness: impact of vaccination age and dose schedule on immunogenicity and cervical cancer prevention – Frontiers, https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2025.1544220/full
- [28]. Guideline for Human Papillomavirus (HPV) Vaccine Use – American Cancer Society, https://www.cancer.org/health-care-professionals/american-cancer-society-prevention-early-detection-guidelines/hpv-guidelines.html
- [29]. (PDF) HPV co-infection in HIV-positive individuals: Epidemiological trends and public health implications – ResearchGate, https://www.researchgate.net/publication/384822420_HPV_co-infection_in_HIV-positive_individuals_Epidemiological_trends_and_public_health_implications
- [30]. (PDF) The impact of HPV/HIV co-infection on immunosuppression, HPV genotype, and cervical cancer biomarkers – ResearchGate, https://www.researchgate.net/publication/388708087_The_impact_of_HPVHIV_co-infection_on_immunosuppression_HPV_genotype_and_cervical_cancer_biomarkers
- [31]. Factors associated with HPV and other self-reported STI coinfections among sexually active Brazilian young adults: cross-sectional nationwide study | BMJ Open, https://bmjopen.bmj.com/content/9/6/e027438
- [32]. (PDF) Impact of human papillomavirus and coinfection with other sexually transmitted pathogens on male infertility – ResearchGate, https://www.researchgate.net/publication/384019232_Impact_of_human_papillomavirus_and_coinfection_with_other_sexually_transmitted_pathogens_on_male_infertility



Related news
Hepatitis C: Do Not Ignore It!
Hepatitis C is a liver inflammation caused by the Hepatitis C virus (HCV). You can contract the virus through contact with infected blood. Most people with HCV have no symptoms. Crucial Fact: There is currently no vaccine for Hepatitis C. The best prevention is avoiding high-risk behaviors. However, testing and treatment can prevent complications and […]
Hepatitis B: A Comprehensive Guide
Hepatitis B is a liver disease caused by the Hepatitis B Virus (HBV). Infection can be short-term (acute) or long-term (chronic). One in two people with Hepatitis B do not know they are infected. HBV is highly contagious and spreads through contact with infected blood and body fluids. Vaccination is the best way to prevent […]
The Invisible Enemy: Chlamydia in Women and the Silent Threat of Infertility
Most of us tend to think that if there are no unusual symptoms, the body is perfectly healthy. However, the truth is that there is an invisible ‘enemy’ silently hiding in your body, capable of causing serious consequences, even infertility. That is Chlamydia, one of the most common sexually transmitted diseases (STDs) in women. Chlamydia […]

Urinary Tract Infection-UTI
Urinary Tract Infection (UTI), also known as urinary tract infection or urinary infection, is one of the most common infections globally, affecting millions each year worldwide, with a significant financial burden on society. The disease occurs when bacteria invade any part of the urinary system, including the kidneys, ureters, bladder, and urethra. Although usually treatable, […]

Syphilis Testing: Current Methods, Pros & Cons, and What You Need to Know
Syphilis is one of the common sexually transmitted infections (STIs) that can progress silently but leave serious consequences if not detected and treated promptly. Regular syphilis testing helps with early diagnosis, protecting your health and that of your partner. This article will help you understand the current syphilis testing methods, the pros and cons of […]
Persistent Sore Throat That Won’t Go Away? Do Not Ignore It – You Might Have Chlamydia!
Have you ever had a sore throat that dragged on for weeks, visiting multiple doctors without finding the cause? Even antibiotics didn’t help? It is very likely that the culprit is not the flu, a virus, or common bacteria – but a sexually transmitted infection called Chlamydia. Chlamydia doesn’t just “hide” in the genital area. […]

Syphilis Overview
Syphilis is one of the most common and serious Sexually Transmitted Infections (STIs), caused by the bacterium Treponema pallidum. If not diagnosed and treated promptly, the disease can progress through multiple stages, causing permanent damage and threatening life. 1. What is Syphilis?? Syphilis is an infection caused by the spirochete bacterium Treponema pallidum. The disease can […]
Chlamydia: A Comprehensive Overview
Chlamydia is one of the most common Sexually Transmitted Infections (STIs) worldwide, caused by the bacterium Chlamydia trachomatis. It is preventable and curable, spreading mainly through unprotected vaginal, oral, and anal sex. 1. What is Chlamydia? Chlamydia is a common sexually transmitted infection (STI) that can occur in both men and women, caused by the […]

Syphilis in the LGBT Community: Are Signs, Symptoms, and Treatment Different?
1. Syphilis and the LGBT Community? Syphilis is a sexually transmitted infection (STI) caused by the bacterium Treponema pallidum. Although it affects all population groups, the rate of syphilis infection is higher in the LGBT community, especially among men who have sex with men (MSM), due to certain sexual behavioral characteristics and barriers to healthcare access. […]

Can Genital Warts Be Treated at Home?
1. What are Genital Warts? Genital warts, also called venereal warts or anogenital warts, are a common sexually transmitted infection (STIs) caused by the Human Papillomavirus (HPV). Although most HPV infections are clinically asymptomatic, HPV types 6 and 11 are responsible for about 90% of visible genital wart cases. It is important to note that other HPV types, […]
