




Submit your info or message us on Zalo or Messenger
Trichomoniasis: Symptoms, Consequences, Complications, and Diagnosis
Health bulletin
08/08/2025
1. Introduction to Trichomoniasis (Trichomoniasis)
1.1. What is Trichomonas vaginalis?
Trichomoniasis, is a very common sexually transmitted infection (STI), caused by a single-celled protozoan parasite named Trichomonas vaginalis. It is important to note that Trichomoniasis is caused by a parasite, not a virus. It is the most common non-viral STI globally and can be completely cured with medication. Although the disease is curable, the high global prevalence of Trichomoniasis highlights significant challenges in diagnosis, access to treatment, and disease control. Therefore, Trichomoniasis is sometimes considered a “neglected parasitic disease.
1.2. Prevalence and Global Impact
Trichomoniasis is a global public health issue of significant scale. In the United States, an estimated 3.7 million people are infected. Globally, the World Health Organization (WHO) estimated approximately 156 million new T. vaginalis infections among people aged 15–49 in 2020, including 73.7 million cases in women and 82.6 million in men. About one-third of these new infections are concentrated in the WHO African region. Notably, the global incidence of T. vaginalis is higher than the sum of Chlamydia trachomatis, Neisseria gonorrhoeae, and syphilis combined. Disease prevalence shows significant differences among population groups. Infection is more common in women than in men, and older women have a higher risk than younger women. In the United States, the disease is also more common in Black women. These epidemiological patterns are not random; they are linked to factors such as older age, lower education levels, lower socioeconomic status, and multiple sexual partners. Studies also indicate that structural racism has contributed to maintaining this significant disparity in the Black community. Socioeconomic factors and systemic inequalities play a crucial role in determining who gets infected and who is diagnosed and treated. Therefore, prevention and control efforts must be culturally sensitive, address health equity, and focus resources on affected or higher-risk communities and individuals, rather than solely on individual sexual behavior.
1.3. Transmission Methods and Non-Sexual Routes
The parasite Trichomonas vaginalis spreads from an infected person to an uninfected person during sexual intercourse. It is primarily transmitted through genital contact, including vaginal, oral, or anal sex. The most common transmissions are from penis to vagina, vagina to penis, or vagina to vagina. Additionally, it can also spread through skin-to-skin contact in the genital area without ejaculation. Sharing sex toys without proper cleaning or not using a condom can also transmit the parasite. It is important to understand these transmission routes for effective prevention measures and to dispel common myths. Trichomoniasis is not spread through non-sexual contact, such as sharing food or drinks, kissing, or holding hands. Poor personal hygiene is also not a cause of Trichomoniasis, as it is a parasitic sexually transmitted disease. Although there are some rare reports suggesting potential transmission from towels, toilet seats, or swimming pools, in most cases, it is a sexually transmitted disease. Emphasizing sexual transmission while dispelling hygiene myths is critical for delivering effective public health messages. This helps shift the focus from shame or blame to understanding the actual routes of transmission, encouraging testing and treatment without stigma.
1.4. High-Risk Populations
Anyone who is sexually active can contract Trichomoniasis. However, some groups have a significantly higher risk. The disease is more common in women than in men, and older women have a higher risk than younger women. In the United States, Black women also have a higher prevalence. Key risk factors that increase the likelihood of infection include: not using a condom during sexual intercourse, having multiple sexual partners, a history of other STIs, having a new partner or contact with a confirmed infected partner, intravenous drug abuse, and not using any form of barrier contraception. Identifying these specific high-risk groups is crucial for developing tailored public health interventions that go beyond general awareness. For example, women living with HIV are recommended for routine screening for T. vaginalis. Additionally, studies have shown that sex workers are a group with a very high prevalence, at 12.16% in one specific study. Public health campaigns and clinical guidelines should prioritize these groups with targeted screening, education, and service access, as a “one-size-fits-all” strategy will not be sufficient for effective Trichomoniasis control.
2. Signs and Symptoms of Trichomonas Infection
2.1. Symptoms in Women
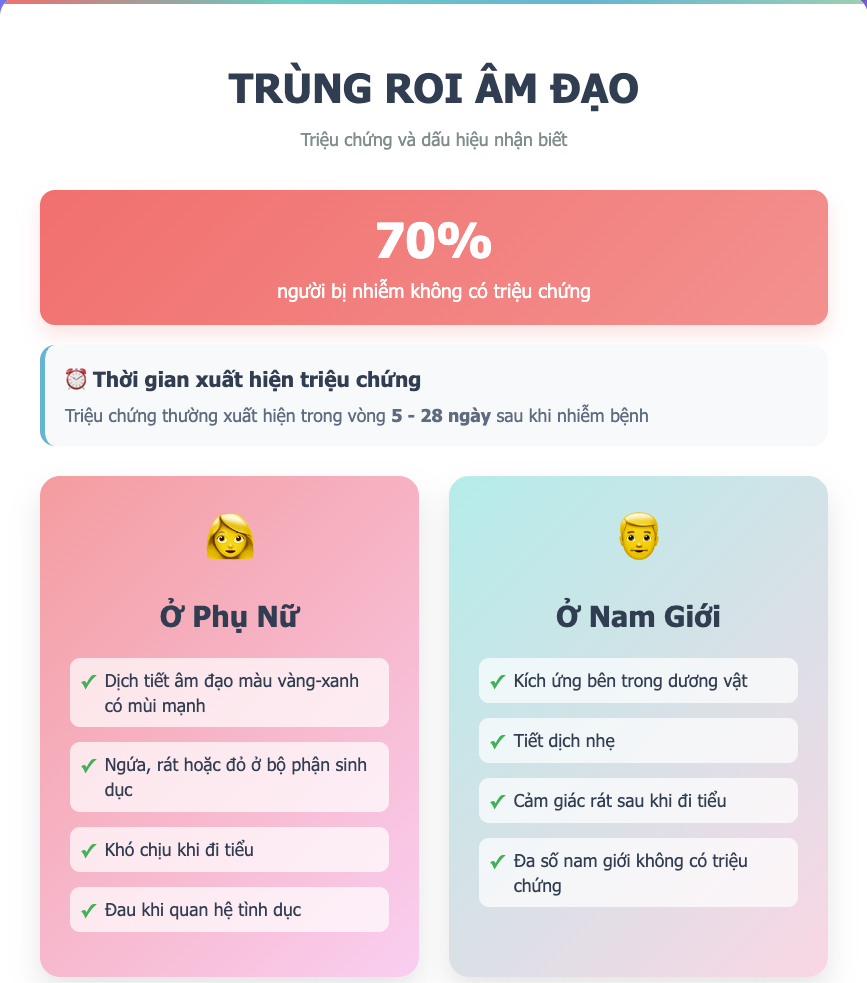
When a Trichomonas infection causes symptoms, they can range from mild irritation to severe inflammation. Symptoms can begin 5 to 28 days after infection, or much later, and may appear and disappear. Common symptoms in women include:
- Abnormal Vaginal Discharge: Often thin or frothy, may be clear, white, yellow, or greenish, accompanied by an abnormal foul odor, often described as a “fishy smell.” Vaginal discharge is the main symptom women may experience, and in some cases, it may contain pus, along with vaginal redness and pain.
- Genital Irritation: Itching, burning, redness, or pain in the genital area, including the vulva and vagina.
- Discomfort during urination and sexual intercourse: A burning sensation or pain during urination (dysuria) and during sexual intercourse (dyspareunia).
- Lower Abdominal Pain: Some women may feel pain in the lower abdomen.
- “Strawberry Cervix”: A characteristic but rare clinical sign is a “strawberry” shaped cervix (colpitis macularis), with tiny red spots on the surface. This sign only appears in about 2-5% of cases.
2.2. Symptoms in Men
Unlike women, most men infected with Trichomoniasis do not have any symptoms. This is an important factor contributing to the spread of the disease. When symptoms do occur, they may include:
- Penile Irritation: Itching or irritation inside the penis.
- Burning sensation during urination or ejaculation: A burning sensation after urination or ejaculation.
- Penile Discharge: Discharge may be clear, pus-like, or frothy.
- Urethritis: Some men may experience urethral inflammation or urethral discharge.
- Less common symptoms: Testicular pain, frequent urination, or cloudy urine. In some cases, Trichomoniasis can cause urethritis, epididymitis, or prostatitis.
2.3. Asymptomatic Status and the Importance of Testing
One of the most challenging characteristics of Trichomoniasis is the high rate of asymptomatic cases. About 70% of infected individuals have no obvious signs or symptoms. This means many people are unaware they are infected and unintentionally transmit the parasite to others. Because symptoms are often vague or absent, Trichomoniasis cannot be diagnosed based on clinical signs alone. The absence of symptoms also allows the infection to persist for months or even years if left untreated. The high rate of asymptomatic infection is the main cause driving continuous transmission and making disease control difficult. This creates a vicious cycle where people unintentionally spread the infection, hindering effective public health control if only relying on symptom-based diagnosis. Therefore, accurate and timely diagnosis requires laboratory testing, especially for high-risk groups, even in the absence of symptoms. Thus, a proactive screening strategy and comprehensive partner treatment are extremely important to break the chain of transmission.
3. Consequences and Complications of Trichomonas Infection
Untreated Trichomoniasis can lead to numerous severe consequences and complications, affecting reproductive health, pregnancy, and increasing the risk of contracting other sexually transmitted infections.
3.1. Impact on Reproductive Health: Vaginitis, Cervicitis, Pelvic Inflammatory Disease (PID), and Infertility
In women, T. vaginalis is a common cause of vaginal discharge and is associated with an increased risk of developing Pelvic Inflammatory Disease (PID). PID is a serious inflammatory condition affecting the uterus, fallopian tubes, and ovaries, which can lead to infertility, increased risk of ectopic pregnancy, and chronic pelvic pain. Trichomoniasis can also cause vaginitis, cervicitis, and urethritis in women. Vaginitis is the most common clinical manifestation in symptomatic women. Additionally, T. vaginalis infection is also linked to infertility in women. Proposed mechanisms include the activation of the host’s immune system, leading to damage and inflammation of uterine and fallopian tube epithelial cells, as well as direct damage to oocytes and interference with ovulation. In men, T. vaginalis infection is also associated with infertility, potentially by impairing sperm motility through binding to sperm glycoproteins, causing phagocytosis and/or hindering the lateral movement of sperm, as well as direct damage and destruction of sperm cells.
3.2. Impact on Pregnancy and Newborns
Trichomoniasis infection during pregnancy is a serious concern as it is associated with adverse pregnancy outcomes. Pregnant women with Trichomoniasis are more likely to have preterm birth (delivering too early) and low birth weight babies (under 2.5 kg). It is also associated with premature rupture of membranes. Although rare, the infection can be transmitted to the baby as it passes through the birth canal, leading to vaginal and respiratory infections in the newborn. The link between Trichomoniasis and adverse pregnancy outcomes like preterm birth and low birth weight emphasizes the need for screening and treatment in pregnant women. Timely diagnosis and treatment are crucial during pregnancy. Metronidazole, the primary treatment drug, is considered safe for pregnant women. However, a notable point is that current guidelines do not recommend routine screening for asymptomatic pregnant women. This indicates a potential gap in public health policy or clinical practice, where the known risks of infection during pregnancy may not be adequately addressed by universal screening. Some experts have suggested that Trichomoniasis should be a reportable condition for pregnant women screening due to these adverse pregnancy outcomes. Healthcare providers should consider individual risk factors for pregnant patients to ensure timely diagnosis and treatment.
3.3. Link with HIV and other Sexually Transmitted Infections
Trichomoniasis infection can significantly increase the risk of contracting or transmitting other sexually transmitted infections. This parasite causes genital inflammation, creating a more favorable environment for HIV infection or transmitting the HIV virus to a partner. Increasing evidence shows that Trichomoniasis enhances HIV transmission. Conversely, people living with HIV may also have a higher risk of T. vaginalis infection. The inflammation caused by T. vaginalis acts as a biological cofactor, significantly increasing the risk of HIV acquisition and transmission. This means the infection is not just a nuisance but creates a biologically conducive environment for the spread of a much more severe STI like HIV. Therefore, treating and preventing Trichomoniasis can be a crucial strategy in the broader fight against HIV/AIDS, especially in areas with high prevalence or in key population groups. Additionally, Trichomoniasis is strongly associated with the presence of other STIs, including Chlamydia trachomatis, Neisseria gonorrhoeae, Treponella pallidum (syphilis), human papillomavirus (HPV), and herpes simplex virus (HSV) types 1 and 2.
3.4. Potential Link with Cancer (Cervical and Prostate)
Studies have indicated a potential link between T. vaginalis infection and the risk of certain cancers. T. vaginalis infection is associated with a higher risk of developing prostate or cervical cancer. For cervical cancer, individuals infected with T. vaginalis have a higher risk, especially when co-infected with human papillomavirus (HPV). This association is supported by meta-analyses. Proposed reasons include a higher rate of co-infection with high-risk HPV types. This suggests a possible synergistic effect where T. vaginalis creates a favorable environment for HPV infection or the progression of precancerous lesions to cancer. This finding reinforces the importance of comprehensive STI screening and management, including HPV vaccination and cervical cancer screening, as part of a holistic approach to sexual health. For men, T. vaginalis infection is also associated with prostate cancer, although studies are inconclusive and remain controversial. Some studies suggest that this parasite may cause proliferation of prostatic epithelial cells and chronic inflammation. The link with cervical and prostate cancer, especially the synergistic effect with HPV for cervical cancer, suggests a more complex and serious long-term impact than previously understood for Trichomoniasis.
4. Diagnosis of Trichomoniasis
4.1. When is Trichomonas Testing Needed?
The diagnosis of Trichomoniasis cannot rely solely on clinical symptoms, so laboratory testing is essential to confirm the infection. Testing is used to diagnose infection in symptomatic individuals. Even in the absence of clear symptoms, testing may be recommended for high-risk women, such as those who have unprotected sexual intercourse, have multiple sexual partners, or have a history of other STIs. Retesting is also recommended after completing treatment to ensure the infection has been completely eliminated and there is no reinfection. When a patient presents for examination, the healthcare provider will discuss their medical and sexual history and conduct a genital examination to look for suggestive signs. However, it should be noted that routine gynecological or urological examination often does not include identifying Trichomoniasis.
4.2. Modern Testing Methods and Accuracy
There are several different testing methods for diagnosing Trichomonas vaginalis, each with its own advantages and disadvantages in terms of sensitivity, specificity, time to results, and cost.
- Wet Mount Microscopy (Soi tươi dịch tiết): This method has traditionally been preferred for women because it is inexpensive and can be performed on-site in the clinic. However, it has low sensitivity (44%–68%) compared to culture. The sensitivity of the wet mount test decreases rapidly, dropping to only about 20% within 1 hour after sample collection. This method is not suitable for men due to very low sensitivity.
- Nucleic Acid Amplification Tests (NAATs): NAATs have very high sensitivity (95–100%) and high specificity (95–100%). They are considered the gold standard in some settings for the diagnosis of T. vaginalis. NAATs are approved by the U.S. Food and Drug Administration (FDA) for use in symptomatic or asymptomatic women using vaginal swab samples (collected by a clinician or self-collected), cervical swabs, urine samples, and liquid-based cervical cytology samples (liquid Pap smear). Some NAATs are also FDA-approved for male urine samples. The shift from wet mount to NAATs as the “gold standard” indicates a major improvement in diagnostic accuracy, which plays a critical role in identifying asymptomatic cases and improving public health control.
- Rapid Antigen Tests (Các xét nghiệm nhanh): Examples include the OSOM Trichomonas Rapid Test, which can be performed on-site and provides results in 10-15 minutes. These tests have a sensitivity of 82%–95% and a specificity of 97%–100%. However, they are mainly for women, and the OSOM test is not recommended for men due to low sensitivity (38%).
- Culture (Nuôi cấy): Previously, culture was considered the gold standard for diagnosing T. vaginalis. This method has a sensitivity of 75%–96% but results often take 3-7 days. For women, vaginal discharge samples are preferred because urine culture is less sensitive. For men, a urethral swab, centrifuged urine sediment, or semen sample is needed.
- Pap Smears (Phết tế bào cổ tử cung): Pap smears are not suitable for routine Trichomoniasis screening or diagnosis due to poor sensitivity. However, if Pap smear results suggest a possible asymptomatic infection, additional tests (wet mount, NAAT, culture, or rapid test) should be performed to confirm the diagnosis.
4.3. Specimen Collection Procedures for Men and Women
The specimen collection procedure for Trichomonas vaginalis testing varies depending on the gender and the type of test used:
- For Women: Samples can be collected from vaginal discharge (by a clinician or self-collected with a swab), cervical swabs, or urine samples.
- For Men: Samples can be collected from the urethra (with a swab), urine (first-void urine sample), or semen.
- Note for Urine Sample Collection: To ensure accuracy, patients should not urinate for at least one hour before sample collection. Approximately 20-30 mL of first-void urine (the first part of the urine stream) should be provided in a clean container.
Table 1: Comparison of Diagnostic Methods for Trichomonas vaginalis
| Diagnostic Method | Sample Type | Sensitivity | Specificity | Time to Results | Main Advantages | Main Disadvantages |
|---|---|---|---|---|---|---|
| Wet Mount Microscopy | Vaginal/Urethral discharge | 44%–68% | High | Minutes | Quick, inexpensive, performed on-site | Low sensitivity, decreases quickly over time, not used for men |
| NAATs | Vaginal, Cervical discharge, Urine (male/female) | 95%–100% | 95%–100% | Hours to 1 day | Highest sensitivity and specificity, detects asymptomatic cases | Higher cost, requires specialized laboratory |
| Rapid Antigen Tests | Vaginal discharge (female) | 82%–95% | 97%–100% | 10–15 minutes | Quick, performed on-site | Lower sensitivity than NAATs, not used for men |
| Culture | Vaginal discharge, Urethral discharge, Urine sediment, Semen | 75%–96% | Nearly 100% | 3–7 days | High specificity, was once the gold standard | Takes a long time, lower sensitivity than NAATs, requires special sample transport |
5. Co-infection and Differential Diagnosis
5.1. Co-infection with other STI Agents
Co-infection with other urogenital pathogens is very common in individuals with Trichomoniasis. A Trichomoniasis diagnosis should trigger a broader STI screening, as the presence of one STI is an indicator of an increased risk for other diseases. Commonly co-infecting pathogens include Chlamydia trachomatis, Neisseria gonorrhoeae, Treponema pallidum (syphilis), human papillomavirus (HPV), and herpes simplex virus (HSV) types 1 and 2. Specifically, women with bacterial vaginosis (BV) are highly likely to be co-infected with T. vaginalis (co-infection rate of 60-80%) and Candida spp. (20-30%). Due to the high co-infection rate, if T. vaginalis or abnormal vaginal discharge is present, testing for other STIs like HIV and syphilis is recommended. All women with BV should also be tested for HIV and other STIs. The high rate of co-infection requires a “syndromic approach” or comprehensive STI panel testing when Trichomoniasis is suspected or diagnosed. Healthcare providers should adopt a holistic screening approach, especially in high-risk populations, to effectively manage STIs and prevent further transmission and complications.
5.2. Which Agents are Trichomoniasis Symptoms Easily Confused With?
Sexually transmitted diseases (STIs) such as Chlamydia, Gonorrhea, and Trichomoniasis often have similar symptoms like abnormal discharge, painful urination, or itching, making differential diagnosis difficult if relying only on symptoms. This emphasizes the need for professional medical diagnosis through testing. Below is a comparison of Trichomoniasis symptoms with some other common intimate area conditions:
Table 2: Differentiating Symptoms between Trichomoniasis and Common Intimate Area Conditions
| Condition | Common Symptoms (Discharge, Odor, Itching/Pain) | Differentiating Features |
|---|---|---|
| Trichomoniasis | Green or yellow, frothy discharge; foul, fishy odor; vaginal pain or burning; inflammation; itching/irritation inside the penis; burning after urination/ejaculation; penile discharge | “Strawberry cervix” (rare) |
| Bacterial Vaginosis (BV) | Thin, homogeneous discharge; fishy odor that may worsen after intercourse; possible pelvic discomfort | Often no clear inflammation; positive Whiff test (fishy odor upon adding KOH) |
| Yeast Infection (Vulvovaginal Candidiasis) | White, thick, cottage cheese-like discharge; vulvar itching or burning | Usually no foul odor |
| Chlamydia | Often few or no symptoms. If present: painful urination, lower abdominal pain, lower back pain, fever, vaginal/penile discharge, vaginal pain during intercourse, bleeding between periods, testicular pain/swelling, rectal pain/bleeding/discharge | More likely to cause testicular pain in men and bleeding between periods in women than Trichomoniasis |
| Gonorrhea | Often few or no symptoms. If present: thick, cloudy or bloody discharge from the penis/vagina; painful urination; heavy menstrual bleeding or bleeding between periods; painful, swollen testicles; painful bowel movements; anal itching; rectal discharge/pain/bleeding | More likely to cause testicular pain in men and bleeding between periods in women than Trichomoniasis |
Conclusion
Trichomoniasis, caused by the parasite Trichomonas vaginalis, is the most common non-viral sexually transmitted infection globally. Although curable, the high prevalence and large number of asymptomatic cases have created significant challenges in controlling the disease. The high asymptomatic rate (about 70%) means many people are unaware they are infected and unintentionally transmit the disease, making symptom-based diagnosis unreliable and hindering prevention efforts. The disease can cause many serious consequences for reproductive health in both men and women, including vaginitis, cervicitis, pelvic inflammatory disease, and infertility. Notably, for pregnant women, Trichomoniasis is associated with adverse pregnancy outcomes like preterm birth, low birth weight, and premature rupture of membranes. Furthermore, Trichomoniasis infection significantly increases the risk of acquiring and transmitting HIV by causing genital inflammation, creating a favorable condition for the HIV virus to enter. The potential link with cervical cancer (especially when co-infected with HPV) and prostate cancer is also a critical aspect of this disease. Accurate diagnosis of Trichomoniasis requires laboratory testing, with Nucleic Acid Amplification Tests (NAATs) currently considered the gold standard due to their high sensitivity and specificity. Treatment with metronidazole or tinidazole is effective, but adherence to the treatment regimen and simultaneous treatment of all partners is necessary to prevent reinfection, a common problem due to untreated partners. Overall, raising community awareness about Trichomoniasis, improving access to advanced diagnostic and treatment methods, along with implementing comprehensive prevention strategies and effective partner management, are crucial steps to reduce the burden of this common yet often neglected disease.
This article is written by Dr Đỗ Hữu Đạt. The doctor has many years of in-depth experience in reproductive and sexual health care.
Related news
Hepatitis C: Do Not Ignore It!
Hepatitis C is a liver inflammation caused by the Hepatitis C virus (HCV). You can contract the virus through contact with infected blood. Most people with HCV have no symptoms. Crucial Fact: There is currently no vaccine for Hepatitis C. The best prevention is avoiding high-risk behaviors. However, testing and treatment can prevent complications and […]
Hepatitis B: A Comprehensive Guide
Hepatitis B is a liver disease caused by the Hepatitis B Virus (HBV). Infection can be short-term (acute) or long-term (chronic). One in two people with Hepatitis B do not know they are infected. HBV is highly contagious and spreads through contact with infected blood and body fluids. Vaccination is the best way to prevent […]
The Invisible Enemy: Chlamydia in Women and the Silent Threat of Infertility
Most of us tend to think that if there are no unusual symptoms, the body is perfectly healthy. However, the truth is that there is an invisible ‘enemy’ silently hiding in your body, capable of causing serious consequences, even infertility. That is Chlamydia, one of the most common sexually transmitted diseases (STDs) in women. Chlamydia […]

Urinary Tract Infection-UTI
Urinary Tract Infection (UTI), also known as urinary tract infection or urinary infection, is one of the most common infections globally, affecting millions each year worldwide, with a significant financial burden on society. The disease occurs when bacteria invade any part of the urinary system, including the kidneys, ureters, bladder, and urethra. Although usually treatable, […]

Syphilis Testing: Current Methods, Pros & Cons, and What You Need to Know
Syphilis is one of the common sexually transmitted infections (STIs) that can progress silently but leave serious consequences if not detected and treated promptly. Regular syphilis testing helps with early diagnosis, protecting your health and that of your partner. This article will help you understand the current syphilis testing methods, the pros and cons of […]
Persistent Sore Throat That Won’t Go Away? Do Not Ignore It – You Might Have Chlamydia!
Have you ever had a sore throat that dragged on for weeks, visiting multiple doctors without finding the cause? Even antibiotics didn’t help? It is very likely that the culprit is not the flu, a virus, or common bacteria – but a sexually transmitted infection called Chlamydia. Chlamydia doesn’t just “hide” in the genital area. […]

Syphilis Overview
Syphilis is one of the most common and serious Sexually Transmitted Infections (STIs), caused by the bacterium Treponema pallidum. If not diagnosed and treated promptly, the disease can progress through multiple stages, causing permanent damage and threatening life. 1. What is Syphilis?? Syphilis is an infection caused by the spirochete bacterium Treponema pallidum. The disease can […]
Chlamydia: A Comprehensive Overview
Chlamydia is one of the most common Sexually Transmitted Infections (STIs) worldwide, caused by the bacterium Chlamydia trachomatis. It is preventable and curable, spreading mainly through unprotected vaginal, oral, and anal sex. 1. What is Chlamydia? Chlamydia is a common sexually transmitted infection (STI) that can occur in both men and women, caused by the […]

Syphilis in the LGBT Community: Are Signs, Symptoms, and Treatment Different?
1. Syphilis and the LGBT Community? Syphilis is a sexually transmitted infection (STI) caused by the bacterium Treponema pallidum. Although it affects all population groups, the rate of syphilis infection is higher in the LGBT community, especially among men who have sex with men (MSM), due to certain sexual behavioral characteristics and barriers to healthcare access. […]

Can Genital Warts Be Treated at Home?
1. What are Genital Warts? Genital warts, also called venereal warts or anogenital warts, are a common sexually transmitted infection (STIs) caused by the Human Papillomavirus (HPV). Although most HPV infections are clinically asymptomatic, HPV types 6 and 11 are responsible for about 90% of visible genital wart cases. It is important to note that other HPV types, […]